Who needs a CMS-1490s?
Form CMS 1490s comes in handy when a patient, who is a holder of Original Medicare insurance (Part A and Part B), wants Medicare to make money compensation for treatment services and medical supplies paid from the patient’s pocket. To notify Medicare, a patient should file CMS Form 1490-s, which is also called Patient’s Request for Medical Payment.
What is the CMS-1490s for?
The CMS Form 1490s is designed in a way to help Medicare agents receive in-depth information about the patient and the case, to determine the claimant's eligibility for compensation.
Is CMS-1490s accompanied by other forms?
Logically, when submitting the Request for Medical Payment, a patient is supposed to deliver the proof of the payment claimed. Consequently, the attachment of an itemized bill authorized by a claimant’s doctor or medical provider must be submitted along with Form CMS 1490s. Also, a person filing a request must think of a detailed explanation to clarify why a medical provider has objected or is unable to deal with the case.
It should also be noted that if another person is completing the CMS-1490s on the patient’s behalf, and they wish Medicare to release their personal information to a third party, the patient has to complete and sign an Authorization to Disclose Personal Health Information.
When is CMS-1490s due?
There are certain time limits for filing the Patient's Request for Medical Payment. The patient is supposed to submit the CMS-1490s form within one calendar year (12 months) from the date when services were provided. As for the processing period, it can take up to 60 days or more to review a request.
How do I fill out the CMS-1490s?
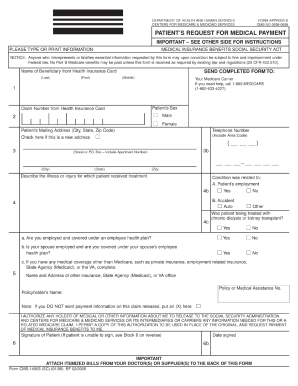
To ensure that Medicare should consider the request without asking for additional information, it is essential that claimants complete CMS-1490s in a full and precise manner. The information required is:
- - Beneficiary's name (copied from the insurance card)
- Claim number
- Patient’s mailing address
- Description of the illness or injury
- Insurance policy data
Where do I send CMS-1490s?
Once the Medicare form CMS 1490s is complete, it should be directed (with a payment bill and statement explaining reasons for the submission) to the local Medicare Carrier office for processing. In case you are not sure where exactly to send the request package, you can call 1-800-633-4227 for an address. It is highly recommended that a claimant keeps a copy of their request for personal records.